Central Sensitization
Central Sensitization and Pain Amplification
Six image-led containers organized from the National Pain Centers central sensitization page: pain categories, the pain-system model, synaptic mechanisms, CRPS imaging evidence, brain reorganization, and stellate ganglion connections.
Pain is the Most Common Reason for Physician Visits
The page opens by framing pain as both a sensory and emotional experience. Central sensitization is introduced before the ketamine discussion because it is the shared nervous-system mechanism behind many painful conditions treated at KIC Pain.
This visual separates major pain categories: nociceptive pain from painful stimuli, neuropathic pain from neuronal damage, inflammatory pain from inflammation, and central pain amplification from abnormal processing by the central nervous system.
- Nociceptive pain: burns, cuts, and tissue injury signals
- Neuropathic pain: nerve or neuronal damage patterns
- Inflammatory pain: arthritis and inflammatory drivers
- Central pain amplification: CNS-based pain processing changes

What is Central Sensitization?
Central sensitization is described as activity-dependent nervous-system plasticity where synaptic strength increases, substantially involving N-methyl-D-aspartate glutamatergic receptors. It can occur after noxious stimuli, peripheral inflammation, or nerve injury in the spinal cord and higher brain centers.
The page explains that central sensitization involves presynaptic and postsynaptic changes, altered transmitter release and action, and synthesis of new neuromodulators. It also resembles memory-like changes in the nervous system, which helps explain why pain sensitivity can persist.
- A stimulus is transmitted to the brain where perception occurs
- Injury can reorganize the pain system and contribute to chronic pain
- Peripheral sensitization begins locally around injured tissue
- Central sensitization involves spinal-cord and brain-level reorganization
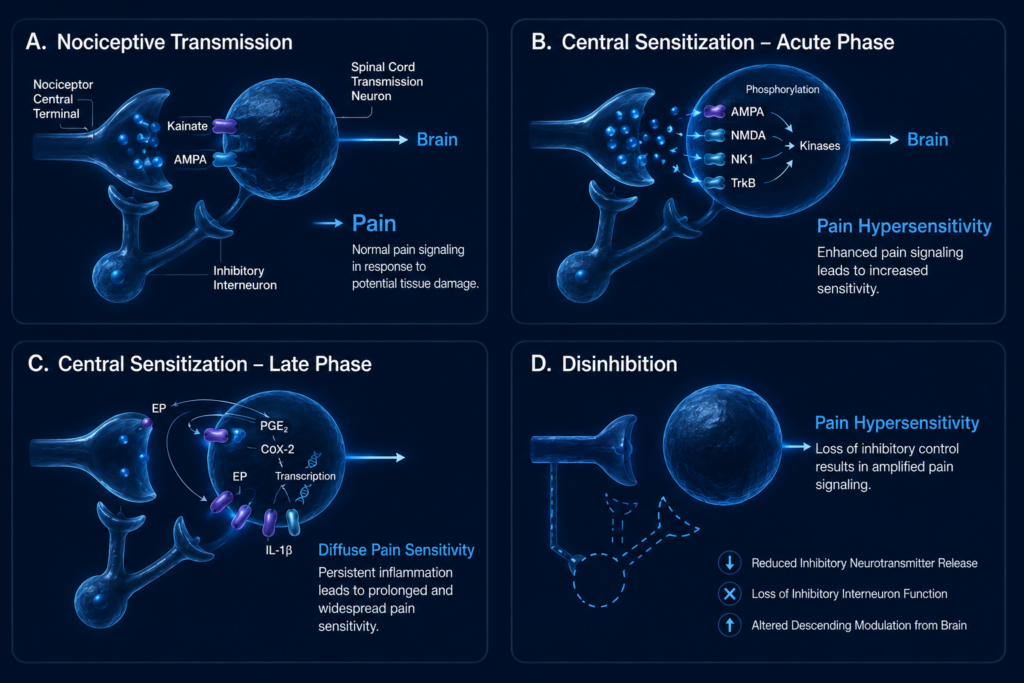
Neurophysiology of Central Sensitization
This image organizes central sensitization into normal nociceptive transmission, acute central sensitization, late-phase sensitization, and disinhibition. The page connects these phases to increased excitability, persistent inflammation, altered receptor activity, and reduced inhibitory control.
Mechanisms highlighted on the page include NMDA receptor activation, altered gene expression in dorsal horn neurons, decreased inhibition, microglial activation, and thalamic and somatosensory cortex changes.
- Acute phase: activity-dependent synaptic plasticity and increased excitability
- Late phase: transcriptional changes and inflammatory mediators
- Disinhibition: loss of inhibitory control amplifies pain signaling
- Result: pain hypersensitivity and diffuse pain sensitivity
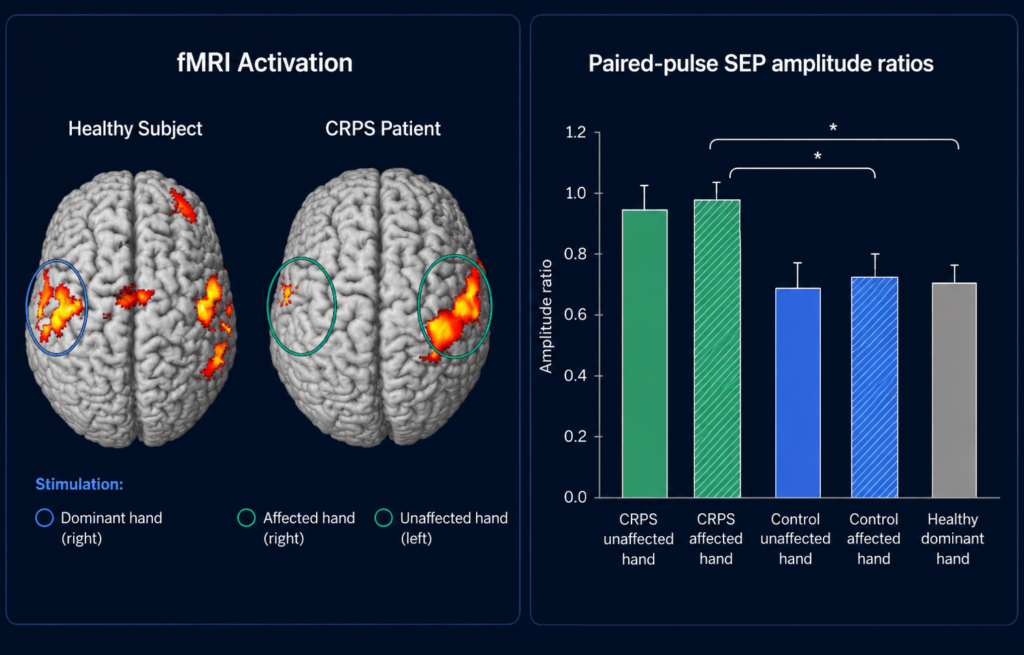
Functional MRI Evidence of Central Sensitization in CRPS
The original page presents fMRI and somatosensory processing evidence in CRPS to show that central sensitization is not only a symptom description. It is associated with measurable nervous-system changes and altered cortical processing.
The page cites work on bilateral somatosensory cortex disinhibition in complex regional pain syndrome type I, reinforcing the relationship between CRPS, altered sensory processing, and central pain amplification.
- Healthy-subject and CRPS-patient brain activation patterns are compared
- Affected and unaffected hand stimulation are shown as separate patterns
- SEP amplitude ratios are used to demonstrate altered sensory processing
- Supports the concept of CNS-level disinhibition in CRPS
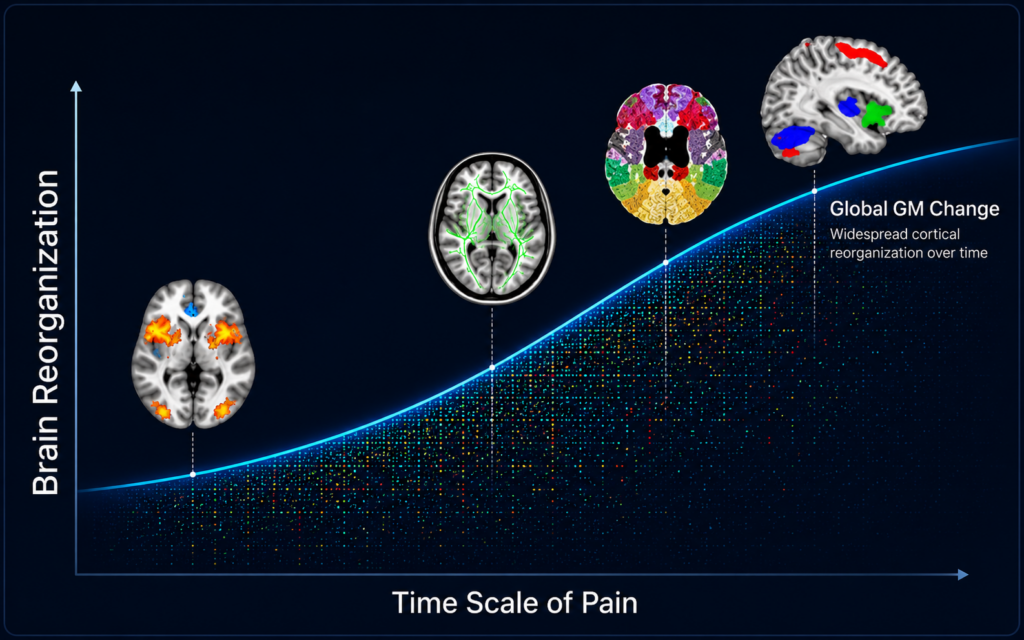
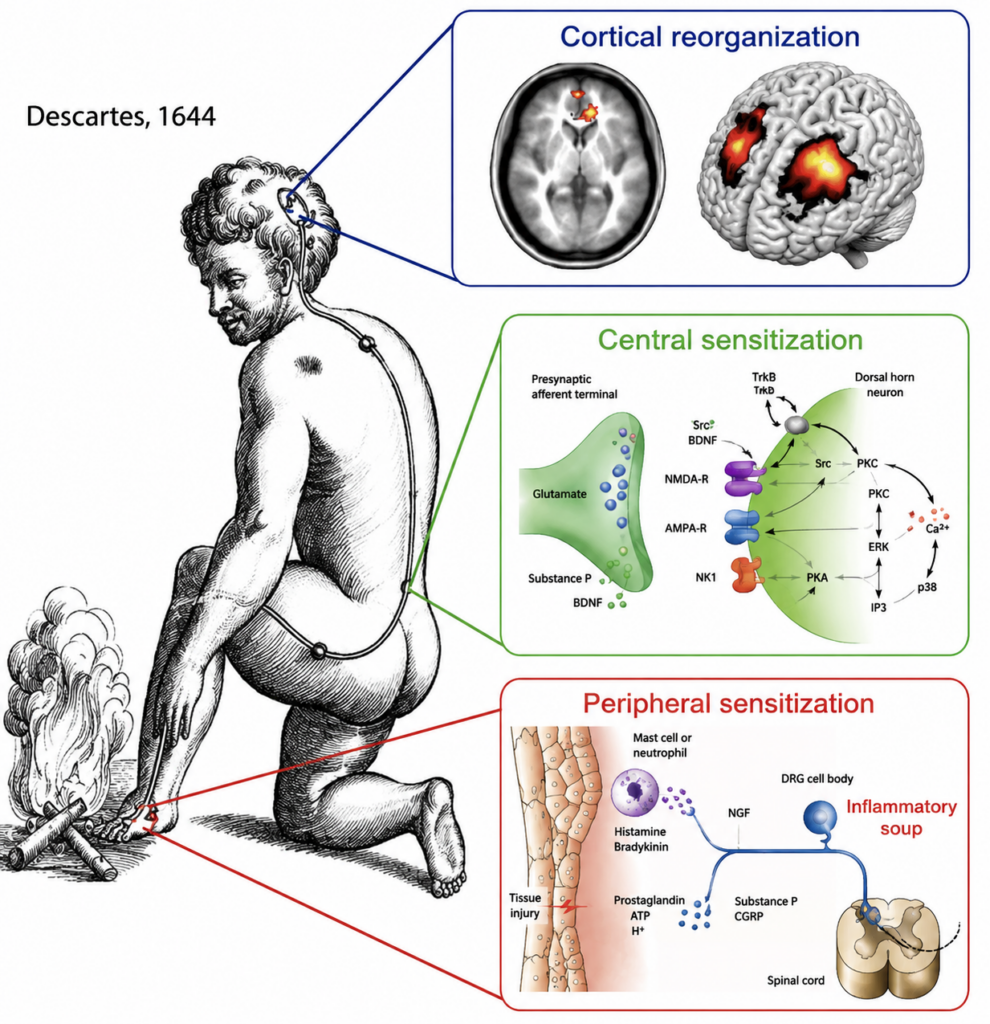
Chronic Pain and Central Sensitization
The page links chronic pain to brain reorganization over time. As pain persists, the central nervous system can become increasingly efficient at generating, amplifying, and maintaining pain signals.
This visual supports the concept that chronic pain is not only a peripheral tissue problem. It can become a brain-and-spinal-cord processing problem, with widespread cortical reorganization and global gray-matter changes over time.
- Pain duration can influence central reorganization
- Persistent input may strengthen pain-processing pathways
- Brain imaging helps explain chronic pain beyond local tissue findings
- Treatment should consider the nervous system, not only the injured body part
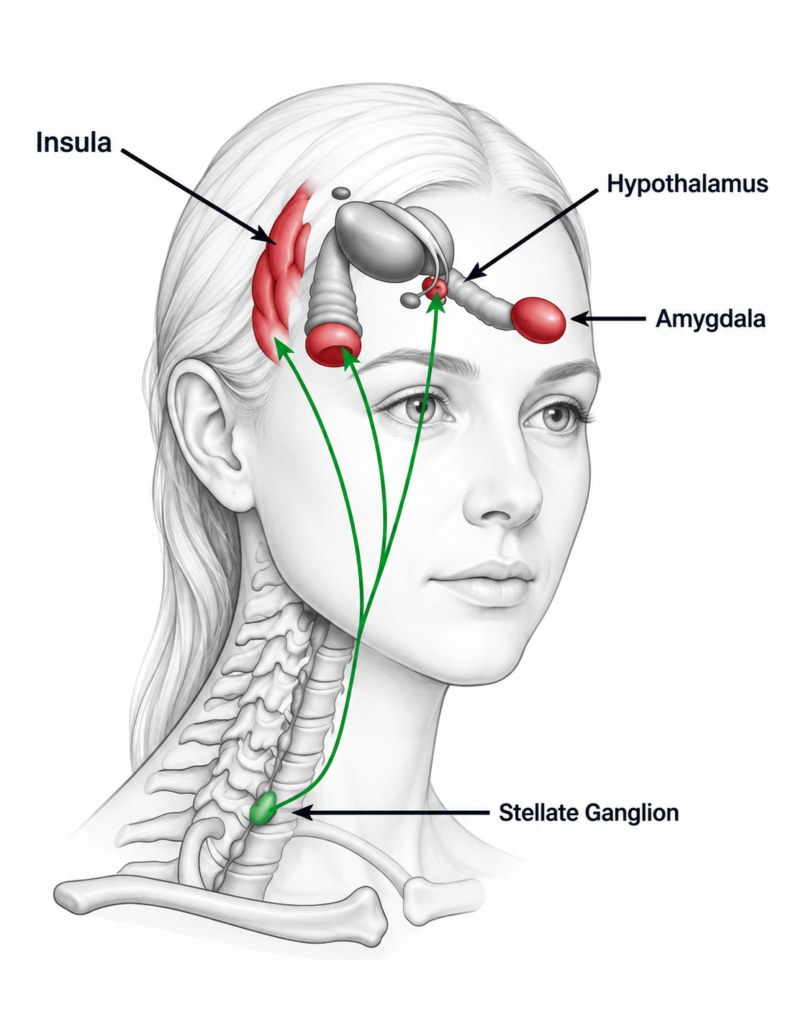
Neural Connection Between the Stellate Ganglion and Central Sensitization
The page explains that neural connections between the stellate ganglion and the hypothalamus, amygdala, and prefrontal regions, especially the insular cortex, may help explain why stellate ganglion block can affect central pain conditions.
The treatment section organizes care into therapy-based, neuropsychological, medication-based, and interventional approaches. Ketamine and ketamine infusion are included among the medication and interventional treatment options.
- Therapy-based: physical therapy, mirror box therapy, graded motor imagery, tactile and sensory discrimination training
- Neuropsych-based: EEG biofeedback, cognitive behavioral therapy, relaxation techniques, and hypnosis
- Medication-based: anti-inflammatories, GABA analogs, ketamine, local anesthetics, SNRIs, vasodilators, and other options
- Interventional: epidural blockade, sympathetic blocks, spinal cord stimulation, IVIG, and ketamine infusion