
Introduction to Ketamine
Understanding ketamine and NMDA receptor modulation.
Ketamine is a non-opioid, non-benzodiazepine, non-paralytic anesthetic with a complex mechanism of action. Its primary clinical relevance in chronic pain is linked to NMDA receptor antagonism, central sensitization, neuropathic pain, and pain amplification pathways.
- First synthesized in 1962 and FDA approved in 1970
- Rapid IV onset with lipophilic distribution
- Primary mechanism: NMDA receptor antagonism
- Relevant to neuropathic pain, wind-up pain, and central sensitization
Drug Overview
Ketamine is a unique anesthetic with pain applications.
Ketamine was first synthesized in 1962 and received FDA approval in 1970. It has been widely used in modern medicine, anesthesia, emergency medicine, battlefield medicine, pediatric surgery, and veterinary medicine.
⚗️
Pharmacology
Ketamine is highly lipophilic and has rapid IV onset. Its IV onset is approximately 30 seconds, with short clinical duration and hepatic metabolism through hydroxylation and N-demethylation.
🧬
Metabolism
Norketamine is an active metabolite, and excretion is primarily through the urine. Clinical protocols should account for safety profile, route, dose, monitoring, and treatment goals.
🛡️
Clinical importance
Ketamine is not an opioid, benzodiazepine, paralytic, or respiratory-depressing anesthetic. This makes it mechanistically distinct from many medications used in pain care.
Mechanism of Action
NMDA receptor antagonism is the central concept.
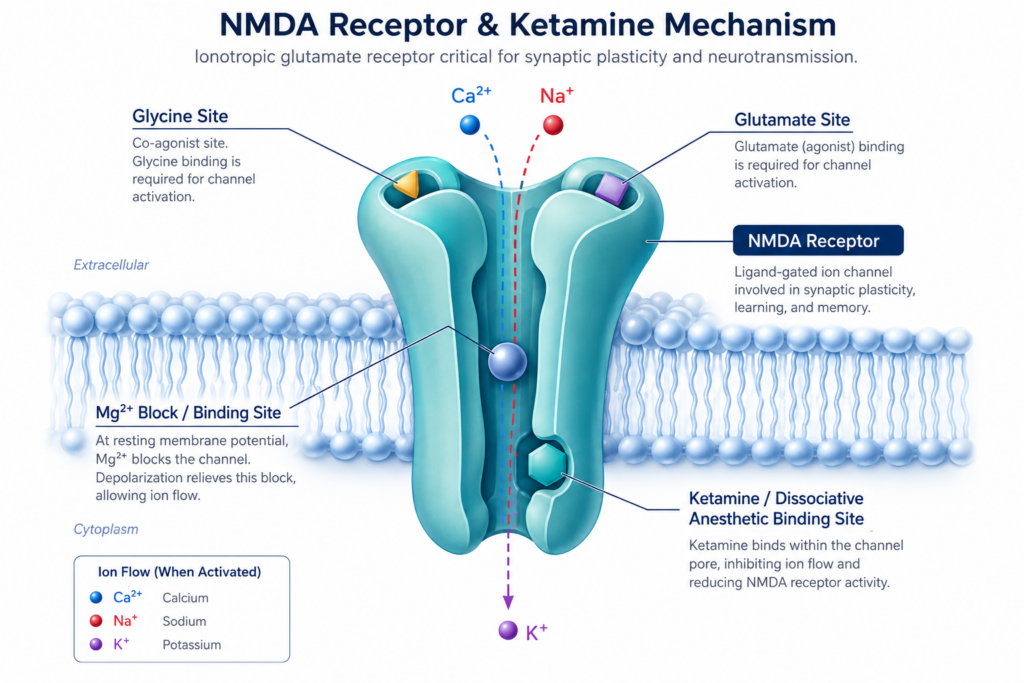
Ketamine’s primary mechanism of action is NMDA receptor antagonism. NMDA receptors are ionotropic glutamate receptors involved in neuronal signaling, gene expression, synaptic plasticity, memory function, and pain processing.
↕️
Ion flow and pain signaling
NMDA channels allow sodium and calcium into the cell and potassium out of the cell. Magnesium blocks the channel under resting conditions.
🧠
Central sensitization
NMDA signaling is closely tied to pain processing, neuronal plasticity, wind-up pain, and the generation of central sensitization.
⚡
Neuropathic pain
NMDA receptor antagonists can reduce neuropathic pain, wind-up pain, and spontaneous pain, which helps explain ketamine’s role in select chronic pain protocols.
Cellular and Chronic Pain Effects
Ketamine affects more than one pathway.
At clinical concentrations, ketamine can influence multiple cellular processes beyond NMDA receptor blockade. These effects help explain why its clinical response can vary by diagnosis, patient biology, route, dosing strategy, and treatment setting.
Receptor and ion-channel actions
- Blockade of NMDA channels
- Effects on HCN1 currents
- Nicotinic acetylcholine ion channels
- AMPA and metabotropic glutamate receptors
- L-type calcium channels
Pain and mood pathway effects
- Delta and mu-opioid receptor interactions
- Opioid potentiation and tolerance effects
- Dopamine and noradrenaline release
- Nitric-oxide pathway effects
- BDNF and mTOR-related synaptic changes
Clinical Pain Context
Why this matters for chronic pain patients.
In chronic neuropathic pain syndromes, some patients experience analgesia that outlasts the active drug level. This may reflect downstream mechanisms involving central sensitization, wind-up pain, glial activation, gene expression, endogenous anti-nociceptive systems, and synaptic plasticity.
- May rapidly reduce select neuropathic pain symptoms
- May reduce allodynia and hyperalgesia in appropriate candidates
- May interrupt NMDA-mediated wind-up pain
- May help reduce opioid tolerance in select contexts
- Requires physician-led dosing, monitoring, and individualized protocols