
Ketamine Infusions
Routes of Administration
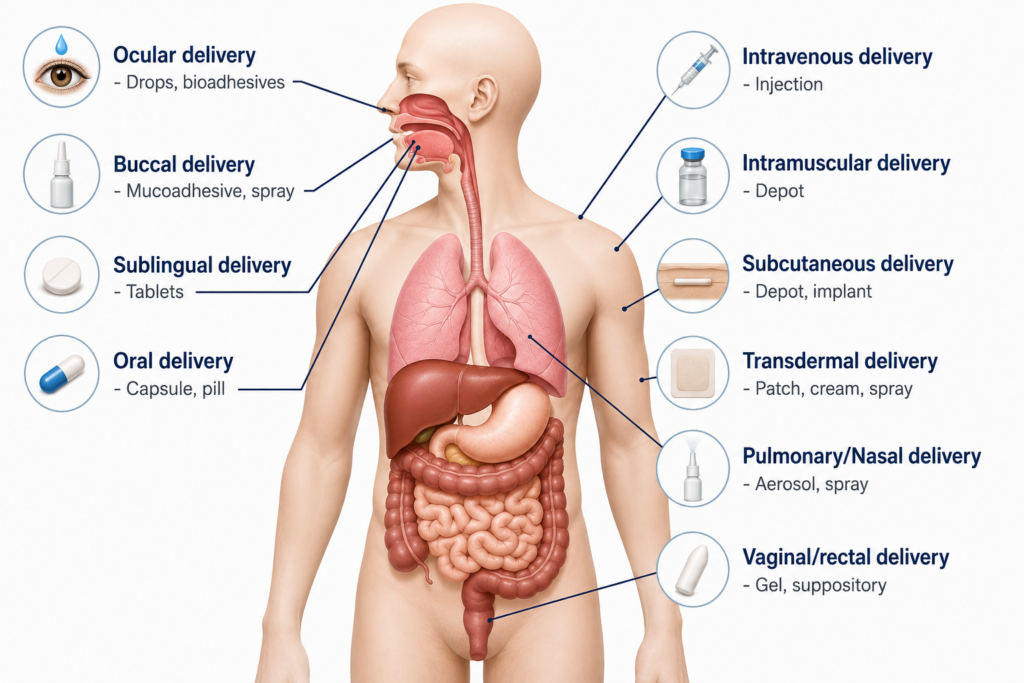
Route of Administration (ROA) refers to the method by which a medication is introduced to the body. For ketamine, the route matters because safety, blood levels, monitoring, effectiveness, side effects, and addiction risk can vary dramatically.
- Infusion (IV)
- Intranasal spray
- Sublingual / under the tongue
- Intramuscular injection (IM)
- Oral / swallowed
- Rectal suppository
Why route matters
The route changes the clinical effect.
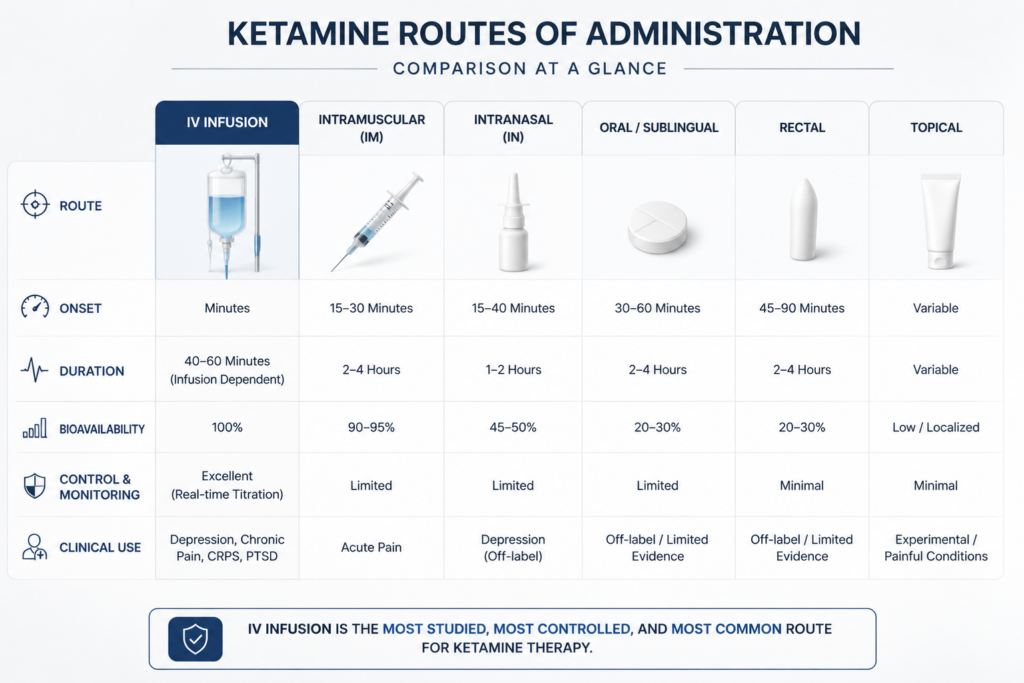
Ketamine may be delivered by several routes, but these methods are not clinically equivalent. The page emphasizes that IV infusion is the most common, most studied, and likely the safest method for ketamine infusion therapy.
The route of administration, together with pharmacokinetics, determines how quickly ketamine enters the body, how steady blood levels become, how closely side effects can be monitored, and how precisely a physician can adjust the treatment.
National Pain Centers emphasizes that ketamine infusions should be performed by physicians who understand both anesthesia-level infusion safety and pain-management strategy, within a comprehensive treatment program.
- ROA affects safety and efficacy
- IV infusion allows steady physician-controlled delivery
- Monitoring is central to ketamine infusion care
- Non-IV routes may create less predictable blood levels
- Treatment should be part of a comprehensive pain plan
Ketamine delivery options
The page lists multiple ways ketamine can be introduced into the body. These routes are included for education, but the clinical message is that IV infusion is treated differently from other methods.
Infusion (IV)
Delivered intravenously at a steady infusion rate. The page identifies IV infusion as the most common, most studied, and likely safest route for ketamine infusion therapy.
Intranasal
Ketamine may be sprayed into the sinus cavities. The page distinguishes intranasal use from monitored IV infusion for central pain conditions.
Sublingual
Placed under the tongue. This route may not achieve the same controlled, steady plasma state as physician-monitored IV infusion.
Intramuscular (IM)
Injected into muscle with a syringe. IM delivery is listed as a possible route but is not presented as equivalent to monitored infusion therapy.
Oral
Swallowed ketamine is listed as a route, but oral use has different pharmacokinetic behavior and monitoring limitations compared with IV infusion.
Rectal
Suppository delivery is listed as another possible route, but the page does not recommend non-IV routes for central pain management.
IV infusion emphasis
Why IV infusion is emphasized
Ketamine infusions work best when delivered at a steady IV infusion rate and paired with carefully selected adjunctive medications. According to the page, when the correct combination is achieved for the patient, reversal of central reorganization can begin to occur.
- Steady infusion rate
- Physician control over delivery
- Monitored clinical environment
- Ability to combine adjunctive medications
- Designed for central pain treatment strategy
- Part of a comprehensive program
Why non-IV routes are not the same
The page states that intranasal, sublingual, IM, oral, and suppository ketamine are not the same as ketamine infusion therapy. These routes are usually not delivered under the same monitored conditions, may not achieve a steady plasma state, and may carry higher side effects, lower efficacy, and greater addiction potential.
- Usually not under monitored infusion conditions
- Steady plasma state may not be achieved
- Peak plasma levels can be dangerously high
- Side effects may be higher
- Efficacy may be lower
- Addiction potential may be higher